

























How art therapy can help children with learning difficulties to understand and communicate their feelings
In recent years, much academic literature has been published regarding art therapy for children with learning difficulties, prompted in part by the increase in the number of art therapists working with these children. However, far less information on the subject has been made available to parents and teachers. Given that art therapy sessions are usually held outside of the classroom setting, it can be difficult for school staff and parents to ascertain the dynamics of what is actually taking place and how art therapists work. This article therefore attempts to demonstrate how art therapy can support children with learning difficulties in educational settings and the ways in which children may derive benefits from it and achieve emotional wellbeing.
What is art therapy?
By definition, art therapy is a form of psychotherapy, which uses art materials and artwork to aid communication. All therapeutic interventions are relation based, but the main difference between verbal and art therapies is that, in art therapy, the artwork and the art making process play a vital part in forming the therapeutic relationship. This allows both the child and the therapist to communicate via the artwork or the art making process in addition to through 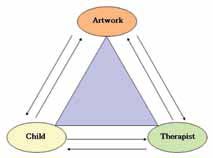 verbal communication (as shown in the art therapy triangle model in figure 1).
verbal communication (as shown in the art therapy triangle model in figure 1).
Unlike art lessons, art therapy does not teach artistic skills, and the primary focus is not on finished products, but on the actual process of art making. Indeed, the artwork created may appear as “unfinished” or even “ugly” in some cases. Artwork made during sessions is not displayed or shown to parents, teachers or the public; instead, it is stored safely and confidentially until the end of the programme. Some children are not able to talk about painful feelings just after making artwork, but may be able to return to these issues when they are ready. It is important, therefore, to keep all of the child’s work until they are ready to deal with it.
Art therapy does not employ psychometric drawing tests, at least not within the UK. The art therapist can contribute as part of a multi-disciplinary team which carries out assessments for a psychiatric diagnosis, but art therapy in itself cannot be used solely as a diagnostic tool for assessment. For example, art therapists are not trained to identify IQs from children’s drawings, although they have a good theoretical understanding of drawing development in children. Similarly, it may be presumptuous to assume that red represents anger or that yellow is associated with happiness (common misconceptions). While this could be the case for some children, it really depends on the context for each individual.
Working with children with learning difficulties
Art therapy can be accessible for children of all ages and a wide range of cognitive abilities. Children may sometimes have difficulty in articulating their feelings and thoughts verbally, but for those with learning difficulties it can be even harder for them to convey their feelings. Art therapy can provide these children with an alternative means of communication. Within educational settings, it enables children to access school life and the curriculum to a greater extent. Alongside the teaching staff, the art therapist can support the child by promoting emotional wellbeing.
When a referral is made, prior to commencement of the programme, the art therapist conducts assessment sessions usually for around four to six weeks. During this period the therapist makes observations regarding body language, how the child engages during the art making process, themes/issues which seem to surface or arise and the ways in which the child is able to communicate with the therapist. After assessment, the therapist makes a recommendation as to the child’s suitability for art therapy, which may be short or long term, on a one to one basis or within a group setting.
There are some specific issues when working with children who have severe learning difficulties. For example, it is common for non-verbal children to use the Picture Exchange Communication System (PECS) or Makaton as a form of communication. On some occasions, the art therapist may have to incorporate PECS into sessions if and when needed. It is also important for the therapist to read all medical documents if the child is on medication or on a special diet. For example, play dough can be made of rice flour instead of normal flour when a child is on a gluten free diet – many children with severe learning difficulties tend to prefer tactile materials such as play dough, and there is a tendency for some to put the play dough in their mouth.
What happens in art therapy sessions?
A typical individual art therapy session is 45 to 60 minutes long, although some young children and children with learning difficulties can only cope with 30 minutes or even less. Normally, sessions are non-directive: the child decides how to use art materials and what to make, if anything. However, some children may need a more directive approach, in particular in the early stages of the programme. In these cases, the child does not have to follow whatever the therapist tells him/her to do, but some tentative suggestions can be made as an introductory activity.
One popular activity is what art therapists call a “drawing conversation”. This was adapted from the “squiggle game” which was introduced by paediatrician and psychoanalyst Winnicott (in his book Therapeutic Consultations in Child Psychiatry, 1971), whose emphasis on the importance of play and creativity remains influential amongst art therapists. I introduce this activity if the child is hesitant to use art materials and seems to need some form of a warm up, in particular at the beginning of the programme. In this activity, the child and the therapist draw on the same sheet of paper. First of all, either the child or therapist makes a mark, which can be a figurative mark or a scribble. Then the other person makes a mark by responding to what has just been drawn, and this exchange is repeated without talking for a few minutes. For example, if the therapist draws a circle, the child may add facial features, and then the therapist may add the body.
 Figure 2 shows a “drawing conversation” between a 13-year-old girl and myself, which was produced during the assessment period. She has an autistic spectrum disorder (ASD) and limited expressive language, and she was extremely anxious in school, which resulted in frequent outbursts.
Figure 2 shows a “drawing conversation” between a 13-year-old girl and myself, which was produced during the assessment period. She has an autistic spectrum disorder (ASD) and limited expressive language, and she was extremely anxious in school, which resulted in frequent outbursts.
In this drawing, she chose a red pen and I used a purple one, and we sat face to face across a table. Initially she copied me: when I drew a straight line side to side, she did too. When I added three dots, she copied me by making three dots. After these exchanges had gone on for about a minute, she then took the initiative and I copied her. This became part of our routine at the beginning of each subsequent session and she always initiated this activity. While children with ASD tend to find this activity difficult, it can gradually encourage them to develop turn taking skills.
As noted above, in art therapy the child uses artwork as a non-verbal method of communication which can be shared with the therapist in a safe environment. Although this is a core concept of art therapy, it is actually rare for the child to make artwork which is directly associated with problems. For example, a child who is sexually abused would be very unlikely to create artwork about an actual incident, but it may be manifested in a subtle way through artwork and body language, and the therapist is trained to recognise such elusive signals.
Case study: communicating through art therapy
In the context of an art therapy session, the therapist may come to understand what the child is communicating other than through artwork per se.
A ten-year-old boy was referred to me for art therapy due to his frequent outbursts and verbal abuse towards staff members. He was born with a rare chromatic disorder, which affected his general development including his verbal communication skills. At the point of receiving a referral, he was “in trouble” on a daily basis as he frequently swore in class.
In art therapy sessions, he often impersonated his class teacher and tried to reconstruct situations where he was told off by her. He rearranged the table and chairs in the room to replicate his classroom. He asked me to sit in the “student” chair and said that I was “him”, while he pretended to be the teacher. He went through what she had said to him, such as “that’s very rude”. He then wrote an apology letter to her, in which the level of his writing skills indicated considerable developmental delay. While he was writing the letter, he said “Mrs xxx doesn’t like me” and “I’m a bad boy”.
What I would like to consider here is how I felt during his role play. This is part of a very complex phenomenon in psychoanalytical theories that are often studied in more depth as a part of an art therapist’s training. This equips the art therapist to analyse and relate to the feelings of the child during the actual art therapy sessions. On this particular occasion, I felt puzzled, isolated and frustrated. Although I could understand that “she” (the teacher) was very angry with “me” (him), I did not know why and it was difficult to follow what “I” (he) was told. I assumed that this was how he might also be feeling in class: puzzled, isolated and frustrated. It seemed that he did not quite understand why he was told off, and he thought that she was angry with him because she didn’t like him. As a result, he became frustrated and threw tantrums and was then told off again; it was a vicious circle. This led me to realise what he was trying to convey, and also helped me to see the big picture regarding what he was going through.
Art therapists are primarily concerned with how the artwork is made, and in this particular case, the child’s apology letter has to be understood in conjunction with the role play. It might not sound like a typical art therapy session, but therapists often work flexibly according to children’s abilities, especially when working with children who have learning difficulties.
 Case study: exploring feelings through art therapy
Case study: exploring feelings through art therapy
This is the story of an eight-year-old girl in a mainstream primary school who was academic, compliant and had always been a good pupil. However, at the age of seven, she had suddenly lost her hearing completely due to sickle cell disease, and she had become very ill. She was wearing hearing aids on both ears and her class teacher communicated with her through a special microphone connected to the hearing aids. Despite experiencing such traumatic change, she appeared to cope well in class and was still achieving a high standard in her school work. However, the SENCO felt that she might need the opportunity to explore her feelings after going through such a tough time, and referred her to art therapy.
During the therapy, she was polite and never showed aggressive behaviours. She rarely initiated talking about her hearing unless it was to inform me that she had to miss a session the following week due to a hospital appointment. Throughout the programme, her artwork was well planned and very neat. She always came with a clear plan as to what to make and showed good concentration skills to achieve what she originally intended to do. However, as sessions went on, it became apparent that she was very self-critical and persevered to achieve the standards she set for herself.
Although her language was always very polite, she became demanding and was always asking for something more than I could provide. On one occasion, she said that she wanted to use blue paint but when given bottles of different blue paints, she said that neither of them were what she wanted. I suggested that she could mix the blue with other paints to make the colour she wanted, but she said that she wanted another bottle. Through such dialogues we discussed the feeling of disappointment that pervades when there is no choice but to accept and acknowledge circumstances, something she has had to experience on many occasions since her hearing loss.
When she made the clay work in figure 3, she said that it was a child sitting on a sofa with a remote control who was watching TV. She did not say that the child was herself, but she said it was how her life used to be. She remained a compliant pupil in class and gave the impression to others that she was coping with her disability. In reality, though, she was still battling with her loss of hearing and was also struggling to find a balance between being “good” and expressing her frustration (which she shared in our sessions). This case demonstrates how art therapy can be used not only with troubled children, but also to provide emotional support for those who might need to explore their feelings in more depth.
Conclusion
This article has served as an introduction to art therapy and how it may be used to help children with learning difficulties. I hope that the clinical examples have provided insight into the types of approach taken by therapists when working through art therapy sessions. It is important to remember, though, that art therapy is one part of a whole team approach, and liaison with other professionals and parents/carers is obviously vital when working with children with learning difficulties.
Further information
Fuyuko Takeda is a state registered art therapist and has worked with children and adolescents in a range of educational settings, including mainstream primary and secondary schools, special schools, a PRU and a children’s home. She is a member of the Art Therapy in School Service:
www.atiss.co.uk
Information about art therapy is available from the British Association of Art Therapists:
www.baat.org












