

























Johanna Barclay explains VERVE video interaction therapy.
Speech, language and communication needs (SLCN) is the most common primary type of need for pupils on SEN support, at 23%. Johanna Barclay and colleagues evaluate the use of video interaction therapy to promote changes in children’s communicative participation.
In 2015, Guy’s and St Thomas’ Community Speech and Language Therapy Service ran a pilot project offering ‘Video, Endorse, Respect, Vitalise, Eye’ (VERVE) contact (Cummins, 2015), with nursery practitioners using goal attainment scaling (GAS) as a measure of children’s progress. This project showed promising results and was well received by practitioners. In this article we present our 2016 follow up study.
What is VERVE?
VERVE is a form of video interaction therapy focusing on developing and integrating communication and learning abilities, with an emphasis on self-regulation and face watching. Parents or practitioners (usually teaching assistants) focus on their timing and skill in interaction, using moment-by-moment video analysis and reflection. Several adult child interaction (ACI) approaches have developed over the past decades (for example, ‘Parent Child Interaction’ (PCI); Palin PCI; and ‘Pre-school Autism Communication Therapy’) with a growing evidence base (including Falkus et al, 2015; Fukkink et al, 2011). In practice, these are sometimes used without video, despite this being central to their effectiveness. McDonald et al (2015) found video feedback was key to increased use of communication-facilitating strategies by early childhood educators. Allen et al (2011) also showed that video interaction therapy could be successful with children with communication difficulties aged eight to 10 years.
VERVE builds on the established ACI approaches, but emphasises the use of video to highlight the fundamental importance of self- regulation and face watching, drawing on neurological research, for example Porges (2011) and Siegel (2015).
Project method
“VERVE
is a form of
video interaction therapy”
After our initial pilot we wanted to investigate whether using VERVE with practitioners in schools leads to clinically significant gains in children’s communicative participation. Using the results of a questionnaire based on The Communication Trust’s ‘Speech, language and communication framework’, we identified five schools to include in the project. Twenty-one primary school practitioners completed a four-week block of sessions, each paired with a different child from nursery up to Year 6 (age range 3 to 11 years).
To track progress we used the ‘Focus on the Outcomes of Communication Under Six’ (FOCUS) (Thomas-Stonell et al, 2012) rather than GAS because of its breadth and established validity. The FOCUS is based on the ‘International Classification of Functioning framework: Children and youth version’ (WHO, 2007) to detect changes in children’s communicative participation. It rates 34 items (for example, ‘My client is comfortable when communicating’) based on observations. All practitioners completed an anonymous FOCUS for the child during the first session to provide a baseline and at a review session three to five months later.
Video analysis
The practitioners met with an SLT for a 20-30 minute introductory session. Following this they shared weekly paired sessions, facilitated by the SLT, over the four-week period. Each week
participants brought in a five-minute video of themselves and the child at play or completing a familiar activity. Video analysis focused on each practitioner’s use of interaction strategies (e.g. silence/waiting for the child to look towards them) using a self-rating tool. Analysis also explored the timing of the child’s communication and the SLT invited the practitioner to experiment further with a particular strategy.
The practitioners reflected on their use of strategies, the impact of these and any changes in the child with regard to regulation, communicative intent, play patterns or language/speech. During the session the facilitating therapist freeze-framed the videos to highlight examples of the child’s emerging skills. At the review session participants evaluated progress, compared the first and final video clips, completed the second FOCUS and provided feedback via a qualitative questionnaire.
Results and feedback
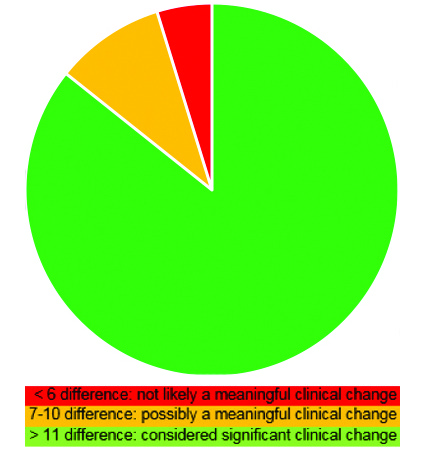
An average of four to six practitioners at each of the five schools completed the programme, targeting 21 different children. Figure one shows the FOCUS total change scores for the 21 children in the study.
The practitioners and special educational needs coordinators (SENCOs) gave qualitative feedback through a written questionnaire based on three themes (see table one below).
Table one:
| Themes | Feedback from practitioners: |
| Impact on the child | “The child I worked with became more open… more face-to-face interaction more frequently.” “I have noticed the child is interacting with other adults around the school. He also has new friends that he speaks confidently with.” |
| Impact on the practitioner | “I was able to identify positive/ negative body language from myself which made me more self-aware and able to consider the impact of both.” |
| Experience of using video | “I felt less self-conscious and found that reviewing the video was helpful… friendly and relaxed sessions helped me to focus on my aims.” |
| Feedback from school SENCOs who supported coordination of the training | “Staff were proactive in reflecting on this themselves, despite not being chased up by the school. They remembered their own goals and continued to work on these.” |
Conclusion and project limitations
The results suggest this project was effective in promoting clinically significant changes in children’s communicative participation over a three to five month period. Based on our clinical experience we feel this is because of VERVE’s focus on the moment-by-moment interactions between the children and the practitioners. Crucially, it gives practitioners a supportive space over consecutive weeks to reflect on their own skills, with the SLT making theory accessible and relevant to the children the practitioners work with, and to celebrate the children’s emerging skills.
Although our project included a small sample size and the absence of a control group, we conducted it within the everyday working school environment. Therefore, it is likely to represent a realistic setting, with findings likely to be representative of routine practice. In addition, we only used one quantitative measure of the child’s communicative participation – a rating scale completed by the practitioner who was not independent and impartial. Future studies should include use of additional objective measures carried out by independent raters.

Author: Johanna Barclay

Johanna Barclay
Johanna Barclay is a speech and language therapist, currently on a two year break from the NHS, working on the small island of St Helena in the South Atlantic. Prior to this she worked with at Evelina Children’s community NHS team in primary schools and the youth offending service in South London for several years.











