

























Srinivas Gada looks at what ADHD is and how best to support individuals living with it
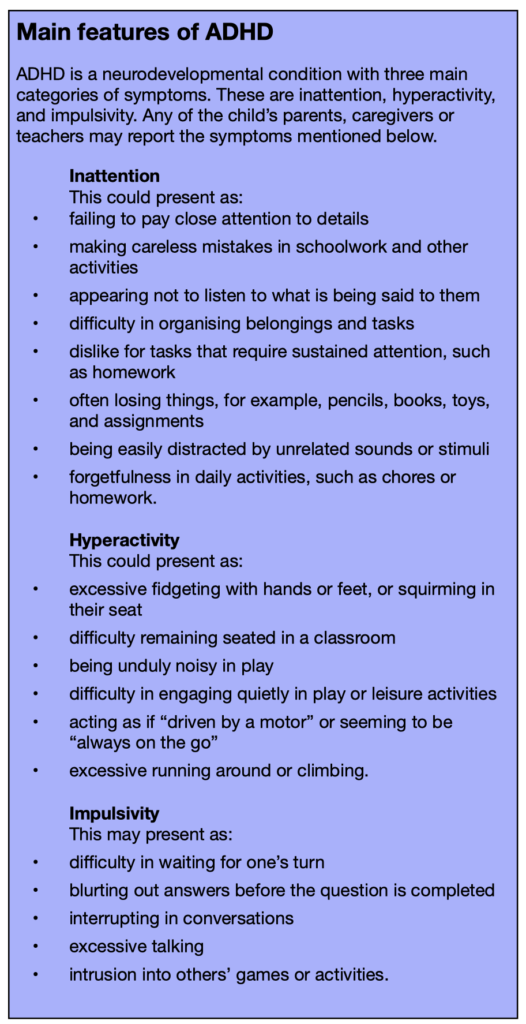
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder. It’s a varied condition of children who are inattentive, impulsive and active at levels higher than expected for their age.
ADHD is thought to affect around three to five per cent of children globally, with prevalence as high as eight to ten per cent of school-age children in the USA. Like most neurodevelopmental disorders, ADHD is more common in boys than girls. This is partly because of identification and reporting bias, as boys tend to show more aggressive and externalising behaviours that are noticeable, and girls tend to show more inattentive and internalising ones, that can be missed easily.
A genetic imbalance of catecholamine metabolism in the frontal brain appears to play a key role in its causation. Various environmental factors would seem to play a secondary role in the causation of ADHD.
Diagnosing ADHD
People who have ADHD, especially if it’s undiagnosed and untreated, exhibit a high rate of low self-esteem, low mood, depression, and anxiety. Attention difficulties can lead to progressive school failure, resulting in poor educational and employment outcomes. These are often avoidable. Untreated ADHD sufferers have a raised chance of injuries, getting involved in accidents and driving offences. Impulsive behaviours can lead to drug and alcohol abuse and assaults, leading to convictions that are preventable.
ADHD can be hard to live with for the person who has it, and for those around them. Children with ADHD are often difficult to bring up and are liable to develop educational, behavioural and emotional issues. The outcome for children and adolescents with ADHD is better if:
- a child is diagnosed and receives help
- caregivers and teachers are given the necessary information, support and advice
- treatment adherence is maintained.
So, the need to diagnose this condition early and manage it effectively is paramount.
The diagnosis of ADHD requires that the child meet the criteria defined by the DSM-5 (APA, USA) or the International Classification of Diseases (ICD-10) criteria for the hyperkinetic disorder. Assessment requires information from more than one setting such as home and school. Additionally, there needs to be evidence of the above symptoms, causing impairment in a child’s social and or educational functioning.
In recent years, researchers and commentators have been keen to point to what are seen to be some of the benefits of having ADHD, particularly in terms of an ability to think creatively and approach knowledge and problems from different perspectives.
How does ADHD affect the child and those around them?
ADHD can affect children and their family and friends in several ways. A child’s difficulty in paying attention can lead to poor school performance. Children with ADHD can be erratic, domineering and intrusive. Overactivity and poor listening skills make it difficult to participate in group activities and team sports. These common ADHD behaviours add to the difficulty in making and or maintaining friendships and could cause peer rejection.
Furthermore, a child’s non-compliant behaviour is often burdensome on parental relationships and teacher-peer relationships. The lack of a “medical label” of ADHD for a child can lead to various moral labels being applied by others to the child or their parents, such as “problem child”, “poor parent” or “difficult family”. All this can lead to social isolation and exclusion from events such as birthday parties.
Consequent to all the above, a child (and their family members) could develop low self-esteem, stress, low mood, anxiety, and depression. These may also lead a child into bullying or being bullied, parental separation, attachment difficulty and or divorce. In some cases, these affect parental employment and family income, leading to suboptimal education and life outcomes for the child.
Things to look out for
Nearly half of children with ADHD could have one or more of the following issues:
- varying degree of learning difficulties or problems with literacy
- coordination disorder or dyspraxia
- difficulties in falling asleep or staying asleep
- autism spectrum disorder (ASD)
- behavioural disorder, such as aggression, conduct disorder and oppositional disorder
- sensory processing disorder (they may, for example, be sensory seeking or exhibit sensory defensiveness)
- mood disorder.
The lack of an assessment for ADHD could lead to a missed chance of the above conditions being identified and successfully addressed.
On the other hand, various other conditions and issues can either present as ADHD or trigger behaviours resembling ADHD. Some of these are:
- sensory impairments in hearing or vision
- sleep impairment
- child neglect or abuse
- autism/ASD
- death or divorce in a family
- parental job loss
- poor parenting or attachment difficulties
- being teased or bullied
- medical conditions such as thyroid disorder, certain epilepsies and anaemia.
On occasions, these conditions can co-exist with ADHD, adding to the complexity of an assessment. Hence a comprehensive evaluation of a child’s medical, psychosocial, developmental and educational aspects is essential before a diagnosis of ADHD can be made.
General principles for supporting children with ADHD
Establishing good communication between home, school and health professionals is vital. During the assessment, allow the child or young person to give their account. Involving the child and family in decision making should help secure their cooperation in executing the management plan.
I would also encourage parental participation in local and national self-help and support groups. Support parents by providing them with information on positive parenting techniques, encouraging a balanced diet and regular exercise for the child. I am not aware of any evidence for the effectiveness of exclusion diets. However, the elimination of foods that worsen behaviour would be beneficial.

ADHD management without medication
Treatment of ADHD involves behavioral/psychological, educational and environmental interventions. Any coexisting conditions should be treated/addressed concurrently with ADHD. For children aged under six years, who meet the diagnostic criteria for ADHD, behaviour therapy rather than medication is advisable. Medication may need to be added if target behaviors do not improve with behavioral therapy alone and if the child’s functioning continues to worsen.
Behavioural or psychological interventions could consist of:
- reinforcing the wanted behaviour (positive reinforcement)
- discouraging the behaviour you don’t want (negative reinforcement)
- setting house rules, routine, structure and timetable and giving visual cues
- avoiding trouble by offering opportunities for play, planning ahead and problem-solving
- offering training and support to parents
- offering the child social skills training.
Educational and environmental interventions could consist of:
- pastoral support
- encouragement
- giving regular feedback to the child
- certain modifications such as sitting in the front of the class, away from windows and doors
- offering short breaks between activities
- working one-to-one or in small groups
- participation in a support group
- access to the resource base
- access to work and taking tests in less distracting environments
- receiving a private signal from the teacher as a reminder
- providing additional time to complete any assignments and tests.
ADHD management with medication

When medication is prescribed for ADHD treatment, stimulant medication such as Methylphenidate is indicated as a first-line agent. Non-stimulant medication such as Atomoxetine is indicated where there are side effects or poor response with the use of stimulant medication. Children being treated need to be monitored regularly according to NICE guidance.
Where the use of medication is being considered by professionals, all concerned need to be provided with good information regarding what the medication options are, their effects, possible side effects, the implications of carrying and storing controlled medications, and issues such as airport laws and taking medication away on holiday.
Coexisting neurological or medical conditions, such as tics or sleep disorder, also need to be managed concurrently.
About the author
Dr Srinivas Gada is a consultant paediatrician in neurodevelopment and neurodisability who has edited the Oxford Handbook of Community Paediatrics. A former consultant at Oxford University Hospitals, he now has an independent practice at the Manor Hospital in Oxford and the Portland Hospital in London.
Website : ocnd.co.uk
LinkedIn : linkedin.com/in/dr-srinivas-gada/













